
Evidence of ginger's potentials against COVID-19
Highlights
• Hyper-inflammation and direct SARS-CoV-2-mediated impacts promote tissue damage.
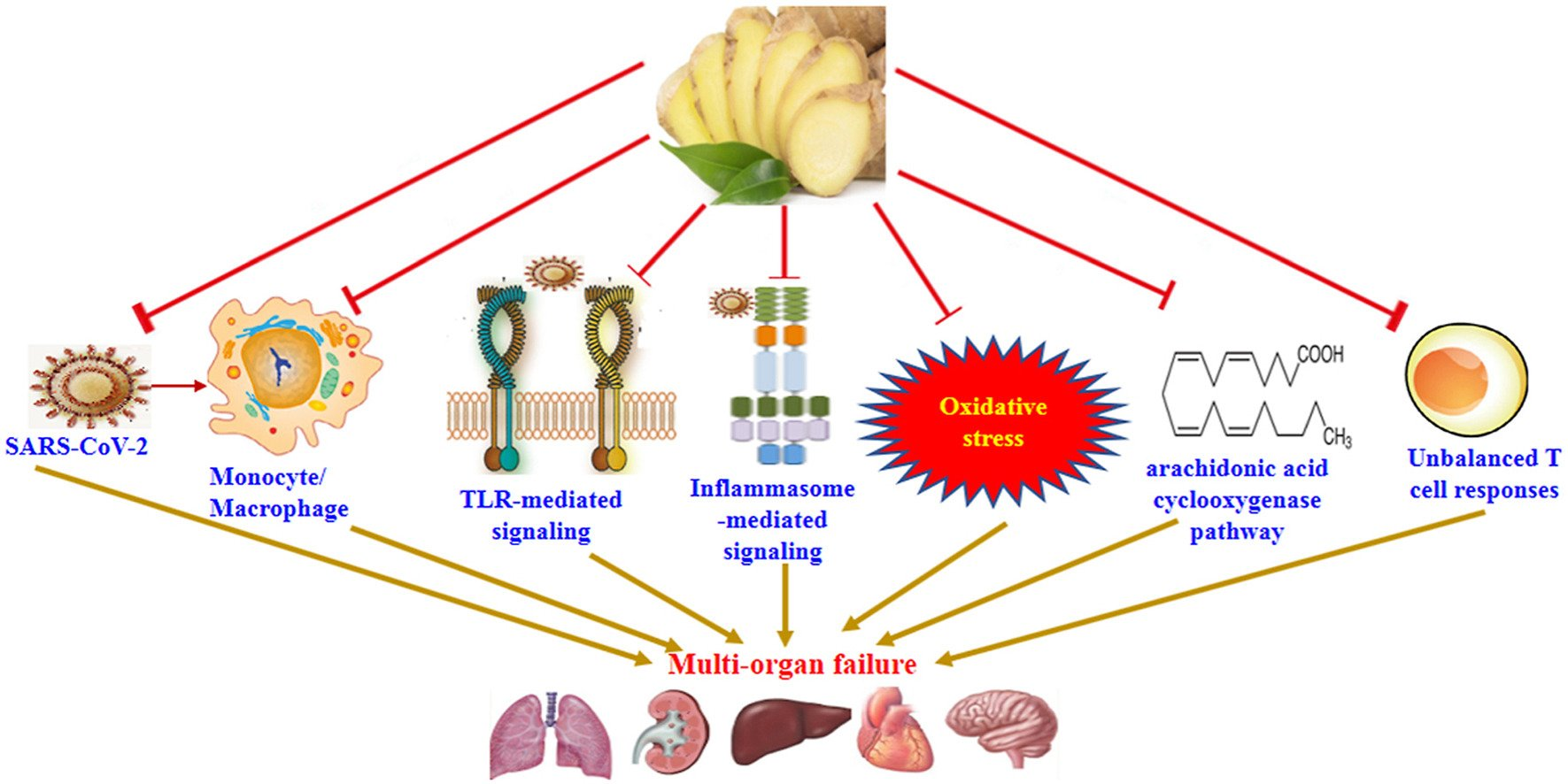
• Ginger can exert anti-SARS-CoV-2 effects and interferes with inflammation.
• Ginger modulates oxidative stress and prostaglandins as harmful factors in COVID-19.
• Unbalanced responses of effector T cells contribute to the COVID-19 pathogenesis.
• Ginger is capable to modulate improper effector T cell responses in COVID-19.
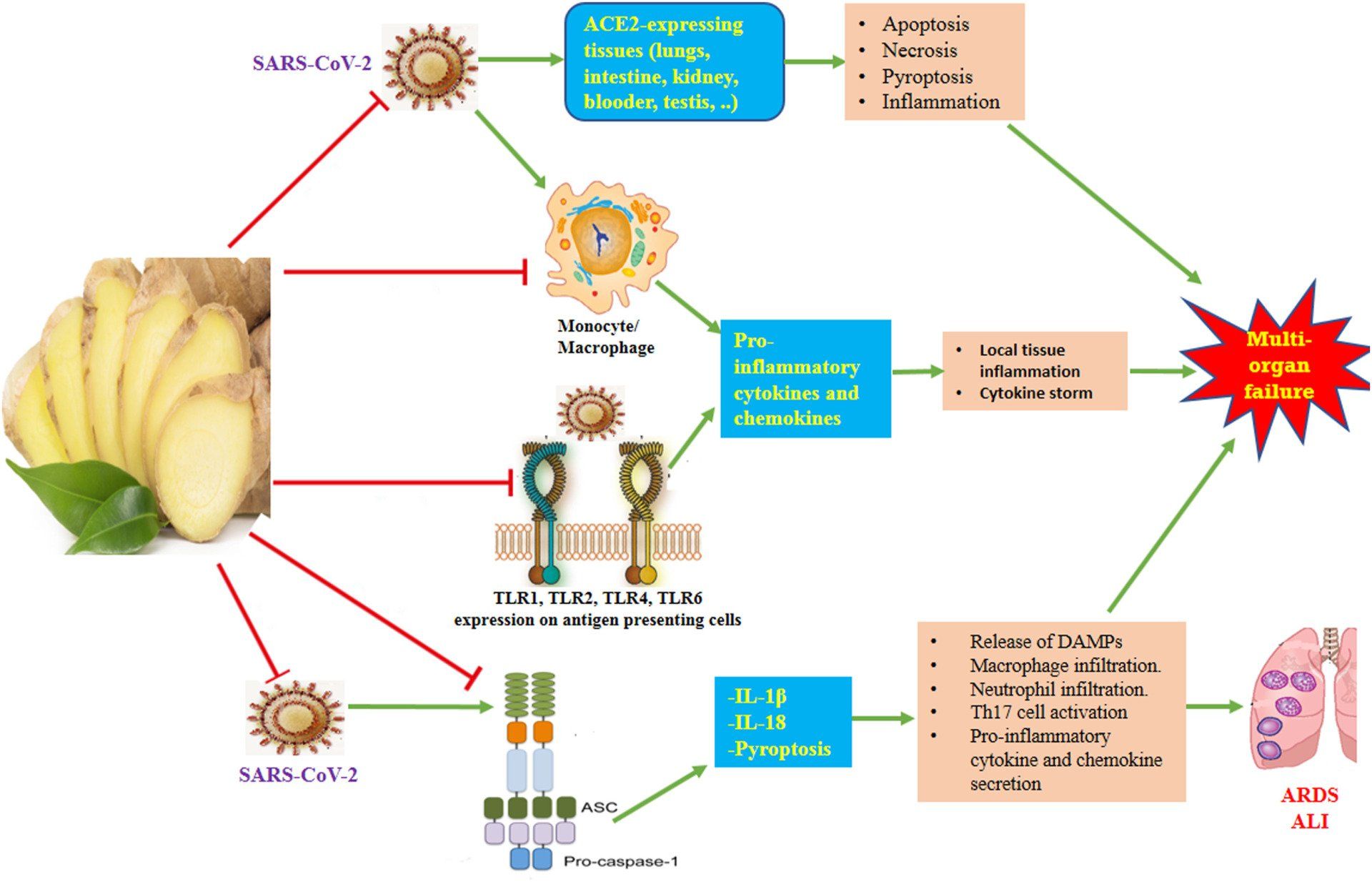
In addition to the respiratory system, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) strikes other systems, including the digestive, circulatory, urogenital, and even the central nervous system, as its receptor angiotensin-converting enzyme 2 (ACE2) is expressed in various organs, such as lungs, intestine, heart, esophagus, kidneys, bladder, testis, liver, and brain. Different mechanisms, in particular, massive virus replication, extensive apoptosis and necrosis of the lung-related epithelial and endothelial cells, vascular leakage, hyper-inflammatory responses, overproduction of pro-inflammatory mediators, cytokine storm, oxidative stress, downregulation of ACE2, and impairment of the renin-angiotensin system contribute to the COVID-19 pathogenesis. Currently, COVID-19 is a global pandemic with no specific anti-viral treatment. The favorable capabilities of the ginger were indicated in patients suffering from osteoarthritis, neurodegenerative disorders, rheumatoid arthritis, type 2 diabetes, respiratory distress, liver diseases and primary dysmenorrheal. Ginger or its compounds exhibited strong anti-inflammatory and anti-oxidative influences in numerous animal models. This review provides evidence regarding the potential effects of ginger against SARS-CoV-2 infection and highlights its antiviral, anti-inflammatory, antioxidative, and immunomodulatory impacts in an attempt to consider this plant as an alternative therapeutic agent for COVID-19 treatment.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is an enveloped virus with single-stranded, positive-sense RNA in its genome, which has affected more than 212 countries and territories.1 SARS-CoV-2 has four fundamental structural proteins, which are called spike (S), nucleocapsid, envelope and membrane proteins, as well as a number of accessory proteins, among them the surface-exposed S protein plays a principal role in the attachment of the virus to its target cells.2 The S protein has a receptor-binding domain (RBD) that binds to its receptor, angiotensin-converting enzyme 2 (ACE2), which is expressed in various organs, such as lungs, intestine, heart, esophagus, kidneys, bladder, testis, liver, and brain.3,4 The brain vascular endothelial cells express ACE2, which provides a direct path for the entry of SARS-CoV-2 into this organ.5 Therefore, in addition to the respiratory system, SARS-CoV-2 can infect the digestive, cardiovascular, urogenital, and nervous systems.3,6
The COVID-19 symptoms, including dyspnea, fever, nonproductive cough, pneumonia, fatigue, and myalgia emerge following an incubation stage of 2–14 days.7,8 Clinically, the symptomatic types of COVID-19 include the following: the mild form (80.0%), which exhibits non-specific minor signs that do not progress to more severe disease; the moderate form (15.0%), which displays localized lung inflammation and pneumonia with or without hypoxia; and severe infection (5.0%), which exhibits systemic hyper-inflammation and acute respiratory distress syndrome (ARDS) with the risk of fatal outcome in critical cases (1–2%).9 Various pathways, in particular, massive virus replication, extensive apoptosis and necrosis of the lung-related epithelial- and endothelial cells, vascular leakage, hyper-inflammatory responses, overproduction of the pro-inflammatory mediators, cytokine storm, oxidative stress, ACE2 downregulation, and impairment of the renin-angiotensin system contribute to the COVID-19 pathogenesis.10,11
Currently, no specific therapy such as relevant anti-viral drugs is available for COVID-19. Herbs can provide valuable sources of components that have immunomodulatory, anti-inflammatory, anti-oxidative and antiviral properties, exerting beneficial effects on the systems that are affected by the virus.12 Experimentally and clinically, ginger (the rhizome of Zingiber officinale) has exhibited numerous therapeutic activities, including anti-inflammatory, antioxidative, immunomodulatory, antimicrobial, anti-fungal, anticancer, neuroprotective, antimigraine, hepatoprotective, hypo-cholesterolemic, cardiovascular protective, respiratory protective, anti-obesity, antidiabetic, anti-nausea, and anti-emetic effects.13 Ginger also displays direct anti-viral effects,14‒19 and can have a protective role against ARDS,20,21 which is the major cause of mortality in patients with severe COVID-19. Thus, ginger can have beneficial impacts on many organs that are affected by SARS-CoV-2 infection. This review provides evidence concerning the potential effects of ginger against SARS-CoV-2 infection and underlines its antiviral, anti-inflammatory, antioxidative and immunomodulatory impacts in an effort to consider this plant as an alternative therapeutic agent for COVID-19 treatment.


Effects of moxibustion for COVID-19 convalescence A protocol for systematic review and meta-analysis

